Ordinarily, you will have had a diagnosis made or suspected by your usual General Practitioner with whom we work in close partnership. Your GP will then refer you on after you request to be seen privately. This process is the result of Arthroplasty Surgery being secondary care and works well in getting you to see the right person for more specialised care more effectively. However, direct self-referrals are also accepted (but may not be accepted by your insurance Company – please check if you are following this route and are not self-funding).
You will then be seen by Mr Woodnutt in what is called a Consultation. As a new patient this will last about 30 mins and will start with you describing your problem and being asked specific questions. There will then be a functional examination (which usually does not need you to undress – but a chaperone is available if you require this).
For some patients, this is followed by an x-ray examination which can be performed on site.
There will then be offered a diagnosis and a possible choice of treatment options. If this includes a recommendation for surgery, you will be informed of the general and specific risks of the type of surgery being offered in your case. This is called the consent process, and this conversation is merely the start of this. Remember the decisions will always be yours (and not the surgeon’s or relatives’ as we are only able to help you make your decision).
You must not make up your mind straight away as you will need time to digest what has been explained and offered and more likely than not, you will come up with sensible questions later on which will need to be answered. It does not matter if you do not think of all the questions you would like to ask at the time – there is always an opportunity to ask at another time! If you cannot make up your mind, it means you have not had enough time to consider the options, or information, or both!
Proceeding to surgery is always a balance as to what would be likely to happen if surgery wasn’t undertaken. Do not panic you will not be the first to have to make decisions and there is always a solution!
Whatever your circumstances, or your degree of knowledge even if you are an old hand at having other joints replaced, a Joint Replacement (or Arthroplasty) is a big operation and should not be undertaken lightly.
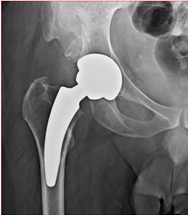
A joint replacement is just that, your old joint is removed and a new “prosthetic” one implanted in various manners and forms.
The main indication for Joint Replacement Surgery is pain. Not because you want to run a few more miles per day or play better tennis (otherwise I would have had one years ago)! It should be remembered that whilst a hip replacement is probably one of the most successful surgical procedures ever undertaken in terms of changing your life back to where it was before your symptoms started and keeping it that way for many years, it is still a big operation and could not only go wrong (through no-ones fault) but it is irreversible.
However, when they do go wrong, such as with dislocation or infection, it is possible to remedy the situation in most cases. But we’d rather not have to! Things which can reduce risks are ardently followed and new methods of improving joint replacement surgery are always being reviewed and tried (under controlled conditions).
For example, surgery is performed by a highly trained team (anaesthetists, anaesthetic assistants, scrub nurses surgical practitioner’s, healthcare workers, radiographers and radiologists, ward teams and administrative staff as well as, of course, Mr Woodnutt) with many, many years of experience and who are all very familiar with sterile working practices.
The importance of this experience cannot be over-stressed: a well-oiled team can deal with any complications which may occur quickly and effectively – in many cases without actually talking to each other such is the degree of understanding and synergy of the team.
Only prostheses of the highest quality are used with the extensive data on their performance and continual communication with the manufacturers is a vital part of the evolution of the prostheses and how they are used. (Mr Woodnutt has been involved in development work of many prostheses over the years and continues with research in this field).
Minimal duration of surgery is important to reduce “open wound time”: this reduces blood loss and risk of infection. This is again achieved by an experienced team with hip or knee replacements often taking as little time as 35 minutes. However, surgery is never rushed, and short-cuts are never taken, speed is a consequence of knowing what you are doing. (A good analogy here is cutting your grass: if you cut your grass every day, your stripes are going to be pretty straight after a month – cutting once a year will leave you spending time looking for the fuel can and wondering how to get around the apple trees!)
Mr Woodnutt has performed nearly 9,000 joints over more than 25 years; many of his team have even performed more than this in their individual roles.
However, risks can never be reduced to zero as there is always a small chance a complication will occur. The full list is given below (which you should read without panicking – they are not compulsory)!
Part of informed consent involves the patient being fully aware of the risks of surgery compared to those which you would have if you did not undergo surgery. You also need to be able to return with questions about risks, particularly in your individual case, and you will not be asked to make up your mind at any time you’re not ready to make your decision. If in doubt, ask us, as very few joint replacements have to be undertaken in a hurry!
The two most serious and common are infection and dislocation (for hip replacements). Infection if it settles around the new prosthesis will almost certainly mean it will have to be removed and replaced when the infection resolves.
Most infections originate from the patient but ambient infection at the time of surgery, cross infection in the ward from staff or visitors or late infection can occur many years later. Rest assured that all staff are trained in reducing this risk to an absolute minimum and extra precautions are taken for higher-risk patients (such as those with diabetes). Currently the overall risk in Mr Woodnutt’s practice is 0.63% (the national average is around 2%).
Dislocation in hip replacements is much less of a problem with modern techniques and prostheses than it used to be in the 80’s and 90’s. Computer simulations for more unusual cases are performed using the Corin OPS system (https://www.coringroup.com/uk/solutions/optimized-positioning-system-ops/). Currently, dislocations in Mr Woodnutt’s practice are less than 0.1% (the national average is around 1%). For knee replacements, it is exceptionally rare.
For knee replacements, the main risk is not so much a complication as a prolonged recovery. The instant pain relief experienced by those undergoing hip replacement is not usually shared by those having a knee replacement. We typically tell patients that you will not thank us until after 6 months! However, in 10% of patients, we know they will not be “happy” at a year, but the good news is that the majority of these unhappy patients will become happy eventually without further surgical intervention. The risk of this occurring is difficult to diminish but certainly not operating too soon is a fairly good piece of advice in most cases!
List of commonly occurring or Serious Complications following joint replacement surgery.
The following is not an exclusive list, but all have an incidence of considerably less than 2%.
Infection (deep infection may mean the joint has to be removed)
Dislocation (much more common in hips than knees but rare with modern techniques and experienced surgeons)
Nerve Injury
Leg Length Discrepancy (in hips more than 1cm; rare after total knee replacement)
Deep Venous Thrombosis (clots in the deep veins of your legs)
Pulmonary Embolus (clots in your lungs which can be life-threatening)
Early failure (such as loosening)
Fracture
Continued or new persisting pain
Bleeding (it is rare that you will need a transfusion after surgery, we usually save and return your own blood).
Heart Attack
Stroke
Death (sudden death following surgery is extremely rare but has to be mentioned here as it is a “seriously occurring event”).
If you are unsure if any terms or consequences of these risks in your particular case, please ask.
Just like the advances in surgery, anaesthesia has progressed to develop an incredibly safe process over the last 10 to 20 years and complications from anaesthesia are even rarer than those mentioned above for the surgery.
There are many different forms of anaesthesia, and you will have the opportunity to discuss these prior to surgery.
In general, unless you have strong wishes, I would thoroughly recommend letting the anaesthetist, who is a specialist in his own right, undertake the procedure of his or her choice. Afterall, he or she would probably choose the most successful method in their hands!
The two most commonly performed anaesthetic procedures are the General or Spinal method. However, the distinction has become less over time, and you may receive a mixture of techniques.
One way or another, you will not experience pain during the procedure, and this allows the surgeon to do the best job!
After surgery, the anaesthetist will play a prominent role in pain relief. Unfortunately, not all pain can be removed after a hip replacement, for example, patients have described a feeling as if they have been kicked in the “behind” by a horse! Not having had this misfortune, I cannot describe it further but the original nagging, underlying joint pain will have usually gone.
The most important aspect of pain management post-operatively is to have confidence that things will get better and the more you move, the better! (We also have a whole cupboard full of goodies, if needed)!
It is a fact that you should soon be better than you were before surgery.
This is very variable but generally is shorter after hip replacements than knee replacements. In both cases, you should expect 3 months' absence from work – longer if your occupation is particularly manual or safety-sensitive (such as climbing ladders or driving commercially).
During the first few days, you will notice a big improvement, progressing from a frame to crutches under the guidance of the physiotherapists and being able to negotiate the stairs before you are discharged.
There are no medals for overdoing it or being too ambitious but likewise, if you don’t perform the exercises given to you, especially for knee replacements, you will suffer in the long term!
You will usually be in the hospital for 2 or 3 days and on crutches in some form for 6 weeks. You will not be able to drive a car for this time (check with your insurance; you do not need to inform the DVLA about your surgery). If we use clips to your wound, these will be removed by one of our team at 5 days after surgery.
We give you medication to reduce developing clots in your legs (DVT) for up to six weeks but after which the risk is very low, and you are usually a lot more mobile.
It may be about 3 months before you forget that you’ve had a hip replacement and it will usually be 6 months before we let you return to sky-diving, surfing, rugby (and space travel). The same applies for knee replacements but do not be upset if it takes a little longer for you to feel confident such as with a golf swing - everyone is different, and you will not have “failed” if you take a little longer as everyone is different.
It is useful (but not essential) to have a friend or relative available for the first few weeks to help with shopping and in emergencies. However, if you live alone, many grocery stores now offer delivery at home, and we can help with an “at-home physiotherapy” service if needed. You will be taught how to negotiate the stairs or steps you may have before you leave the hospital.
Something rarely asked about (but always thought about) is sex! The general rule here is that you should only partake when you feel comfortable, but it is not likely to affect your joint replacement. We would usually advise to have a rest from “such exercise” for about 6 weeks following surgery.
A common question concerns kneeling following knee replacement surgery – particularly for those needing to do this for religious reasons. This may be difficult: few patients will comfortably kneel following a knee replacement if very happy in all other respects. After a hip replacement, it is probably better to kneel on the side you have had the surgery as you can do this without bending the hip too much. (Most mosques will permit the use of chairs for those with a physical need).
We are always on hand should you have problems or concerns, and we will usually see you at 6 weeks following surgery for a routine check-up. After that, we would like to see you periodically but indefinitely. Typically, we would contact you one to two years following surgery and then probably every 3 to 5 years for monitoring purposes. Check x-rays are performed on hips before you leave the hospital and at six weeks for knee replacements. Thereafter, it is usually performed at 5 years or if you are having difficulties.
Once you have recovered, there are no restrictions to your activities: you can do exactly what you want!